
Vital Signs Directed Therapy in Practice: Lessons from Tanzania’s ICU Study
Efforts to improve critical care quality often focus on advanced technologies, expanded ICU capacity, or specialised training. Yet some of the most meaningful gains come from strengthening the basics: detecting vital organ dysfunction early and acting immediately.
Research provides one of the clearest demonstrations of this principle. The study Vital Signs Directed Therapy (VSDT) at Muhimbili National Hospital (MNH) in Tanzania shows how a simple, protocolised approach to managing abnormal vital signs can transform care, even in a highly resource-constrained ICU.
Why VSDT?
The team began with a problem familiar across many settings: severely abnormal vital signs were being documented, but often no acute action followed. This gap was not unique to Tanzania; similar patterns have been documented in high-income settings. The issue is rarely staff willingness; it is structural. Competing demands, unclear expectations, inconsistent supervision, and the absence of clear prompts to act protocolised responses mean that deterioration can be recognised but not treated.
VSDT was developed as a pragmatic solution:
Single-parameter danger vital signs trigger immediate action
Nurses are empowered to initiate stabilising treatments without waiting for a doctor
Actions are low-cost, feasible, and established (oxygen, fluids for shock, airway positioning, etc.)
The protocol complements (not replaces) clinical judgement
In essence, VSDT operationalises the core logic of EECC: early, essential, feasible lifesaving care.
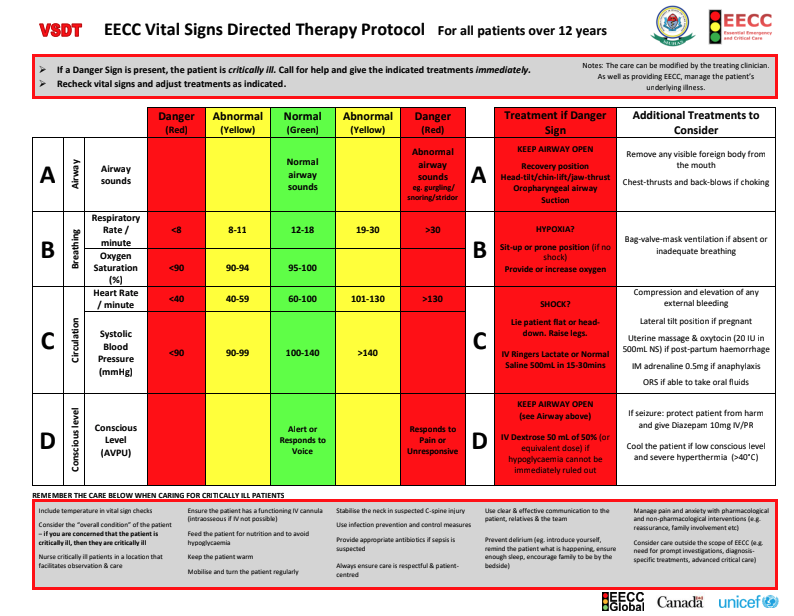
VSDT Protocol for Adults
Implementation in a constrained ICU
The ICU at MNH had six beds, limited physician support, and no formally trained ICU nurses. Despite these constraints, the team delivered a robust implementation strategy:
Co-design with local clinicians
One-day seminars for all ICU staff
Bedside coaching
Local facilitators to reinforce use
Fortnightly remote supervision between Tanzanian and Swedish teams
By formally adopting VSDT as a Standard Operating Procedure, hospital leadership signalled institutional commitment; a crucial but often overlooked factor in implementation success.
What changed?
The study’s findings highlight both the potential and the limitations of protocolised care.
1. Marked improvements in acute treatment
After implementation, the proportion of severely abnormal vital signs that received an acute intervention increased significantly. Staff acted more reliably and more consistently, demonstrating that clear protocols help overcome ambiguity in fast-moving clinical environments.
2. A striking mortality effect in patients with shock
Among patients presenting in shock, survival rose from 8% to 31% after VSDT implementation. This corresponds to numbers-needed-to-treat (NNT) as low as 4.3 to save one life. It reflects the well-established principle that early fluid resuscitation and oxygenation (when appropriately used) can be life-saving. It also shows that controlled fluid therapy in shock in Africa is not dangerous. Recent studies at the time had shown increased mortality of protocols of large fluid volumes.. The VSDT protocol for shock prescribes 500ml at a time, followed by re-evaluation. A practice that is not only safe - but life saving.
3. No overall mortality change for all ICU patients
There was no significant mortality difference when analysing all patients combined. This is an important finding. It highlights that:
The implementation realised a sustained manifold increase in VSDT treatments when indicated (from 23% to 73% at admission and from 3% to 17% in ICU). The dose of VSDT increased substantially, but may still have been too low to realize its full potential.
Some conditions require advanced therapies beyond this ICU’s capacity
Protocols amplify the impact of interventions that are already effective and feasible, but cannot compensate for missing definitive treatments or save patients with irreversible disease.
In short, in this ICU the VSDT protocol maximises the benefit of what is available; but does not replace what is absent.
What can clinicians and health systems learn?
1. Protocols are strongest where effective treatments already exist
Whilst essential interventions (oxygen, fluids, airway support) can change physiology rapidly, where this equipment is available, VSDT produced clear gains. This aligns with broader EECC evidence: the basics save lives when reliably delivered.
2. Task-sharing is not a compromise, it is a necessity
Empowering nurses to act immediately on danger signs proved both feasible and safe. In many settings, waiting for a doctor is neither realistic nor justifiable when deterioration is time-critical.
3. Implementation strategy matters
The co-design process, staff engagement, repetitive training, and supervisory structure were integral. Without these, uptake would have been minimal, a common problem in quality-improvement efforts. This was confirmed two years after implementation, when adherence to VSDT had increased to 29%.
4. Protocols are part of a wider ecosystem
VSDT works best when embedded within:
Routine vital signs monitoring
Availability of core equipment (e.g., pulse oximeters)
Clear escalation pathways
Supportive leadership
This mirrors the EECC framework: clinical processes and hospital readiness must align.

The EECC Framework
Implications for EECC
VSDT can be seen as a forerunner and practical expression of EECC principles. It shows that:
Essential care can be operationalised in real-world settings
Improvements that save lives do not require high-cost investments
Gains emerge when systems ensure the basics are always delivered
As countries begin incorporating EECC into national strategies, the Tanzanian experience offers a model: start with clear, actionable processes that enable staff to act early.
Moving forward
Baker’s work demonstrates that improving critical care does not hinge on expanding ICUs. It starts with ensuring that every severely abnormal vital sign triggers a life-saving response, whether in an ICU, a high-dependency unit, or a general ward.
For researchers, the VSDT study highlights the value of intervention designs that blend feasibility, behavioural insight, and simplicity.For clinicians, it reinforces the importance of acting early on deterioration.For policymakers, it shows that scalable solutions already exist, and that strengthening essential care may yield greater population benefit than investing solely in advanced technology. VSDT is likely to be an even more effective way to address deterioration before ICU admission is needed - in general wards.
EECC Global will continue advocating for approaches like VSDT because they embody a fundamental truth: when it comes to saving lives, reliability in the basics is often more powerful than complexity.