
Lessons for the World: How Tanzania Integrated Essential Emergency and Critical Care into National Policy
As the global health community increasingly recognises the urgent need to improve the care of critically ill patients, Tanzania has emerged as the first country to embed Essential Emergency and Critical Care (EECC) in national policy. A new qualitative study published in BMJ Open offers rare, practical insight into how this happened, and what other countries can learn from the process. Drawing on interviews with policymakers, clinicians, researchers and implementation partners, the study distils the steps, strategies and system conditions that enabled Tanzania to move from early discussions of EECC to coordinated national action.
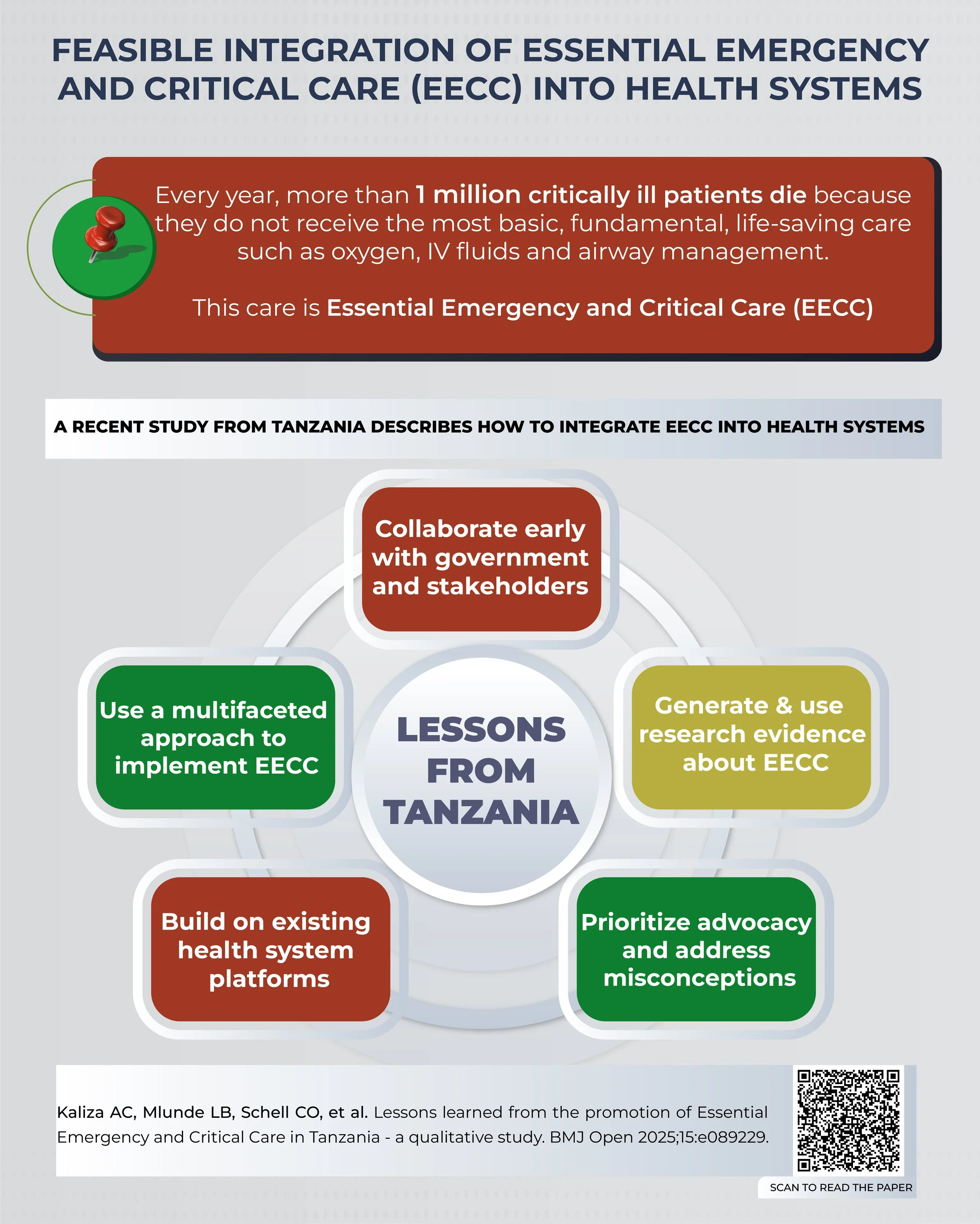
At its core, the research shows that implementing EECC is not solely a technical task. It is a multidisciplinary effort that requires early government collaboration, utilization of research evidence, clear messaging with stakeholders and sustained engagement across every level of the health system. While the Tanzanian experience is shaped by its own context, the lessons are widely applicable to countries seeking to reduce preventable deaths from critical illness.
Why Tanzania Needed EECC
Like many countries, Tanzania faces a high burden of critical illness, much of it occurring outside Intensive Care Units. Most patients who become critically ill are cared for in general wards, where early identification of deterioration and timely life-saving treatments are often inconsistent. Research from Tanzania and similar settings has repeatedly shown gaps in the availability of essential equipment and delivery of fundamental care such as oxygen, fluids and patient positioning.
EECC provides a structured, feasible way to close these gaps. By focusing on simple, low-cost, life-saving actions that can be delivered by any health worker, in any health facility, EECC strengthens the foundations of care across the system. Tanzania’s Ministry of Health recognised this potential, but translating recognition into policy and practice required coordinated effort.
How Tanzania Made Progress: Five Lessons
The first lesson from the study is the critical importance of early and continuous engagement with government. Researchers and clinicians worked closely with the Ministry of Health from the outset, and EECC champions within the country maintained EECC visibility amid competing priorities. Partnerships with organisations such as UNICEF supported the development of a National Strategic Plan for EECC.
Second, research and evidence were central to building understanding and political will. Baseline studies documenting gaps in critical care, alongside emerging health-economic analyses showing EECC's affordability, gave policymakers concrete reasons to act. Evidence served not only to highlight the problem but also to demonstrate that a scalable, cost-effective solution existed.
Third, the team had to address misconceptions about EECC, a challenge familiar to anyone working in global critical care. Many stakeholders initially believed EECC was already being delivered, or that it was synonymous with ICU-based care. Clear messaging was essential to explain that EECC focuses on foundational, life-saving care across all health settings, complementing rather than replacing advanced care.
Fourth, Tanzania’s progress was accelerated by leveraging existing initiatives and external events, particularly the COVID-19 pandemic. The crisis exposed system-wide weaknesses in oxygen access, monitoring and emergency preparedness, creating a natural opening for EECC. EECC principles were integrated into COVID-19 technical guidance and aligned with ongoing programmes in maternal health, paediatrics, emergency care and oxygen scale-up.
Finally, the study emphasises that EECC implementation requires a multifaceted, system-wide strategy. Training alone is insufficient. Equipment alone is insufficient. Real change came from coordinated action involving national policymakers, regional leaders, hospital administrators and frontline providers. The process was adaptive, iterative and required perseverance; but it ultimately led to the formal integration of EECC into national policy.
A Model for Other Countries
Tanzania’s experience shows that strengthening the care of critically ill patients does not depend on high-tech equipment or specialised units. It depends on getting the basics right, at scale, across the entire health system. By combining evidence, collaboration, advocacy and system-wide strategies, Tanzania has demonstrated a pathway that other countries can adapt.
As more nations focus on universal health coverage and equitable access to life-saving care, EECC offers a pragmatic, cost-effective solution to reducing preventable deaths. The lessons from Tanzania are not just encouraging; they are actionable.